www.istockphoto.com
A Nobel-winning breakthrough and lessons from the pandemic
have cancer researchers rushing to develop and test new vaccines.
Understanding how and why the human body works, and when and why it doesn’t, has led to countless health and wellness breakthroughs—including innovative treat-ments, therapies, medications and vaccines. Breast Cancer Awareness Month, which concluded in October, focused our attention on the impact of the disease, as well as the importance of access to screenings. Another component of Breast Cancer Awareness Month is fundraising earmarked for research. In recent years, more and more of that research has concentrated in an area with which we have all become intimately familiar these past few years: vaccines.

The search for clues on how the immune system might be enlisted in the battle against cancer has intensified thanks in part to: 1) COVID having taught us how to dramatically accelerate the production of new vaccines, and 2) a Nobel Prize-winning discovery that clears the path for new cancer vaccines to be tested. Much of this research has been devoted to understanding cancer itself, particularly the ways in which a tumor’s defenses are able to thwart the immune system. Researchers are not only getting a firmer grasp on how this happens but, just as importantly, how well the human body already eliminates rogue cells as they develop. There is even a word for it: immunosurveillance.
“This is a very exciting time to be an oncologist,” says Clarissa Henson, MD, Chairman of Radiation Oncology at Trinitas Comprehensive Cancer Center (left). “The fields of virology, immunology and oncology have been rapidly joining forces to combat and cure cancer.”
Trinitas patients now have access to a wide range of advanced treatment options such as immunotherapy, precision medicine, and clinical trials—many of which are not available elsewhere—thanks to RWJBarnabas Health’s partnership with Rutgers Cancer Institute of New Jersey, the state’s only National Cancer Institute-designated Comprehensive Cancer Center. Researchers there are focused on translating discoveries directly to patients to reduce the incidence of cancer and improve outcomes.
MUC1
Many of those researchers believe that tumors are formed by cells that have found a way to escape immunosurveillance by “looking” normal—sort of a microscopic cat-and-mouse game going on inside our bodies all the time. If this is indeed the case, then the key to effective cancer vaccines may be learning how both the cat and the mouse do what they do. This information would be used to “teach” the immune system how to recognize the cells that elude it now so that they can be neutralized.
One exciting recent breakthrough, by a team at the University of Pittsburgh, was the identification of an antigen specific to tumors—in other words, a molecule or protein that exists on cancer cells but not on normal ones. Researchers believe this is a critical first step in teaching the immune system what to target. Among the cancers that have this antigen, which is called MUC1, is breast cancer. MUC1is also present on cells related to colon, lung, pancreatic and prostate cancer. That’s quite a list of targets, which explains the excitement in the vaccine community. Initial trials have been focused on preventing pre-malignant lesions, such as polyps, from becoming malignant. A similar trial at Pittsburgh on early breast cancer is already gearing up.

Another branch of cancer vaccine research that holds great promise is the field of neoantigen vaccines. These vaccines address mutations unique to one person’s tumor—a “personalized” vaccine, one might say. A neoantigen vaccine is created using a sample of an individual’s tumor, and is then used to prime that person’s immune system to attack the cancer cells. Trials on melanoma patients have shown great promise, prompting research on a neoantigen vaccine targeting pancreatic cancer. An exciting aspect of these types of vaccines is that, once effective versions have been developed, they could be produced very rapidly thanks to the work that was done to scale up production of coronavirus vaccines.
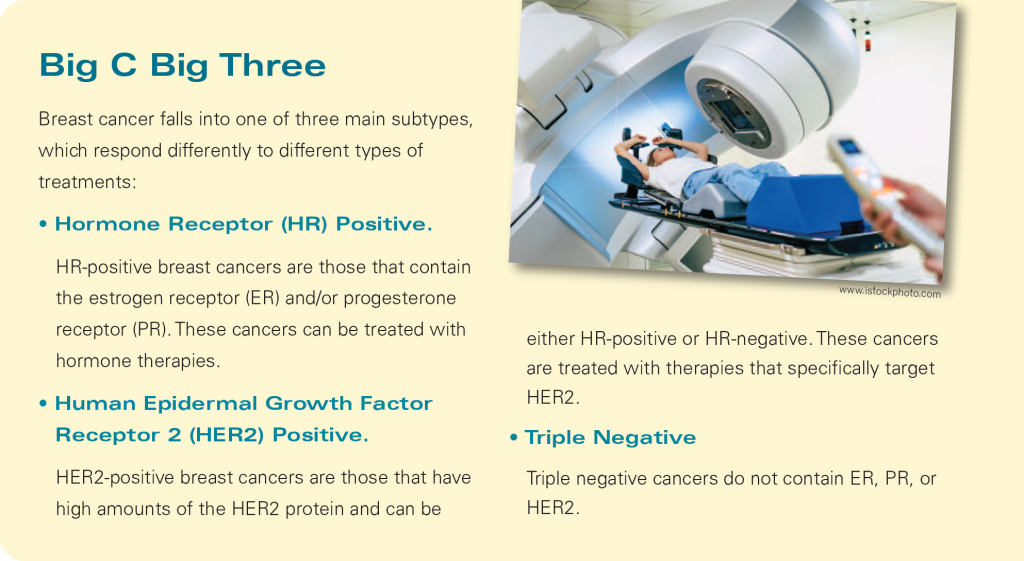
Although it is encouraging to think that we all might have personalized vaccines one day, that may not be necessary because, as mentioned earlier, many different cancers share similar antigens. A case in point is HER2-positive breast cancer, which accounts for about a quarter of all breast cancers and frequently relapses and metastasizes. The HER2 molecule is considered a driver antigen, meaning that it instructs cells to keep dividing. Without these instructions, the cancer cannot grow. A vaccine that prompts the immune system to make its own HER2 antibodies would be a game-changer.

www.istockphoto.com
An early version of that game-changer has already been through initial trials at the Mayo Clinic. A HER2 vaccine was given to 22 patients with invasive breast cancer. Two-plus years later, 20 of the 22 showed no sign of recurrences. It is a small sample, but the results are encouraging. The same team is also working on a vaccine that might prevent breast cancer in women at high risk for the disease.
“We are still learning more every day about the human body and how the immune system fights illness, viruses and cancer,” says Dr. Henson, who adds that the pandemic provided an impetus for some important research, including a study at Emory University.
“Radiation is used to kill both viruses and cancer, UV light is used for sterilization and to kill bacteria and viruses, while higher-energy x-rays are used to kill cancer,” she explains. “During the pandemic, the Emory study showed that low-dose radiation to the lungs in patients with COVID-19 related pneumonia resulted in quicker recovery times, lower rates of intubation and quicker time to hospital discharge.”
Checkpoint Inhibitors
If we are indeed, as top researchers are optimistic, approaching an age of breast cancer breakthroughs, it is due in no small part to an earlier breakthrough that has made research in therapeutic cancer vaccines possible. That would be the development of checkpoint inhibitors, which are now combined with the vaccines given to patients in many test trials.
Chemotherapy suppresses the body’s response to an immunologic stimulus. So, too, does cancer itself. Because cancer vaccines are tested on people with cancer, it can be challenging to accurately gauge the effectiveness of the vaccines. Checkpoint inhibitors stimulate immune checkpoints, counteracting the effects of cancer. This has cleared the path for critical research. In 2018, the Nobel Prize was awarded to James P. Allison and Tasuku Honjo for “their discovery of cancer therapy by inhibition of negative immune regulation.”
Checkpoint inhibitors technically fall under the heading of immunotherapy. Immunotherapy is another area of intense focus that has yielded possible breakthroughs in the fight against breast cancer. An article earlier this year in JAMA Oncology reported work by Korean researchers on a new treatment for HER2-postive breast cancer that works as well as current drugs, but without the often-devastating side effects. Many HER2 patients receive TCHP chemotherapy before surgery with fairly good results; about half go into remission. But TCHP is highly toxic, especially to gastric mucosal cells, which can result in severe diarrhea and even sepsis. It is hard on bone marrow, too. So TCHP is not recommended on elderly patients or women with certain comorbidities.
The Korean phase-2 study replaced carboplatin—the “C” in TCHP—with a monoclonal antibody called atezolizumab and enrolled 67 HER2-positive patients in a yearlong trial. After surgery, patients received more targeted immunotherapy and, at the end of the trials, 61% responded completely. There were still side effects (including immune-related events in 6% of trial participants), but mostly they were aches and pains and some skin conditions.
In other words, another encouraging step in the development of new weapons in the breast cancer arsenal.